Laparoscopic Abdominal Hernia Repair
Modern Keyhole Hernia Surgery

The vast majority of abdominal hernias can now be repaired using minimally invasive (laparoscopic or endoscopic) keyhole surgery. Compared with traditional open surgery, these techniques result in less postoperative pain, smaller scars, faster recovery, earlier return to normal activities, fewer wound complications and, most importantly, a stronger anatomical repair with a lower risk of long-term hernia recurrence.
A/Prof Taylor performs almost all abdominal hernia repairs using minimally invasive techniques because they provide the best combination of durability, faster recovery, improved cosmetic results and reduced postoperative discomfort. Open hernia repair is therefore rarely required in his practice, the only routine exception being small umbilical hernias, which are repaired with simple sutures through a tiny incision hidden within the umbilicus.
Groin Hernias (Inguinal and Femoral)
For almost all groin hernias, A/Prof Taylor performs a laparoscopic Totally Extraperitoneal (TEP) repair.
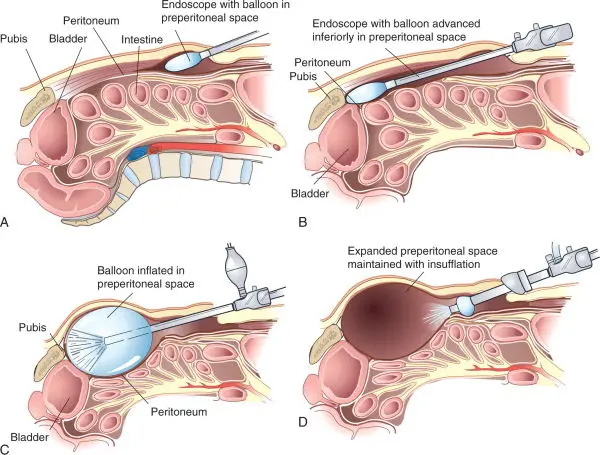
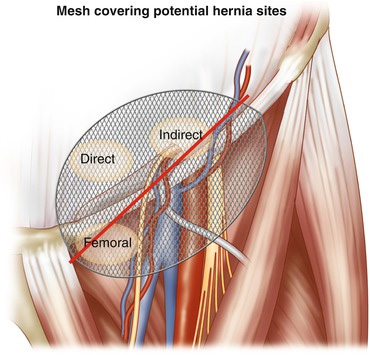
The TEP technique repairs the hernia entirely within the abdominal wall without entering the abdominal cavity. Using three small keyhole incisions, the tissues behind the groin muscles are gently separated to expose the hernia defect. The hernia sac and its contents are reduced, and a large lightweight mesh is positioned over all potential weak areas of the groin. The mesh is held securely within the natural tissue planes and therefore usually requires no additional fixation, greatly reducing the risk of chronic postoperative groin pain.
Because the abdominal cavity is not entered, the TEP approach avoids contact with the bowel and other abdominal organs, resulting in an excellent safety profile and rapid recovery.
TAPP Repair
In selected circumstances, A/Prof Taylor may recommend a laparoscopic Transabdominal Preperitoneal (TAPP) repair instead.
Examples include:
- Recurrent hernias following a previous TEP repair
- Patients who have previously undergone radical prostate surgery
- Selected complex or unusual groin hernias where entry into the abdominal cavity provides a technical advantage
Both TEP and TAPP are performed laparoscopically and reinforce the same anatomical weakness from behind the abdominal muscles using mesh. The choice of technique depends on the individual clinical situation.

Ventral Hernias and Incisional Hernias
Ventral hernias include umbilical, paraumbilical, epigastric and incisional hernias that occur through weaknesses in the abdominal wall.
For most ventral hernias, A/Prof Taylor performs an Endoscopic Retrorectus Repair (eTEP/eRives approach).
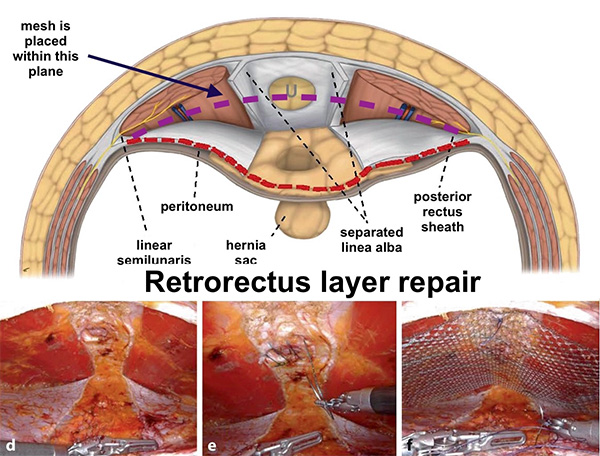
This modern technique reconstructs the normal layers of the abdominal wall by working within the natural retrorectus plane behind the rectus muscles, without entering the abdominal cavity. After carefully reducing the hernia contents, the muscles are restored to the midline and a large lightweight mesh is placed within the retrorectus space.
Positioning the mesh within this anatomical plane provides excellent reinforcement while avoiding direct contact with the abdominal organs. The mesh becomes incorporated into the body's own tissues, providing permanent reinforcement while preserving the natural function and flexibility of the abdominal wall.
The eTEP/eRives approach has become one of the preferred techniques for ventral and incisional hernias because it combines the durability of traditional open retrorectus repair with the advantages of minimally invasive surgery.
Diastasis Recti Reconstruction
Patients with significant diastasis recti often experience abdominal wall weakness, poor core function and abdominal bulging. Many also have an associated umbilical or epigastric hernia that can be repaired during the same operation.
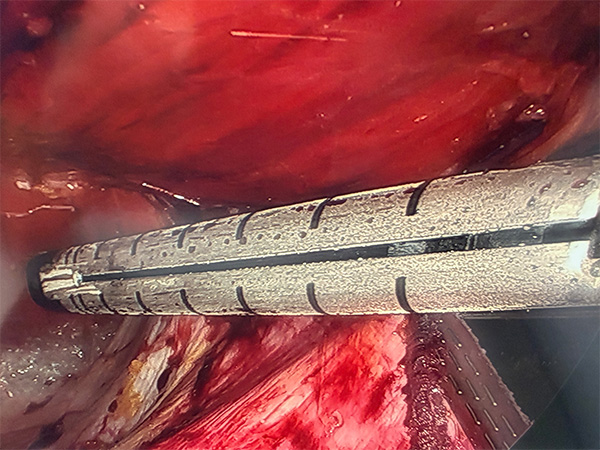
Where surgical reconstruction is indicated, A/Prof Taylor performs a Stapled Endoscopic Retrorectus Reconstruction (eTEP-RS).
This minimally invasive technique restores the normal anatomy of the abdominal wall by bringing the separated rectus muscles back together in the midline. The stretched linea alba is reconstructed to its normal width using a series of tiny linear staples deployed by a sophisticated surgical stapling device, producing an extremely precise and consistent reconstruction.
Long-term strength is then restored by positioning a large mesh within the retrorectus plane, where it becomes incorporated into the body's own tissues, providing permanent reinforcement while preserving the natural function of the abdominal wall.
Compared with traditional open reconstruction, this approach achieves excellent cosmetic results through small keyhole incisions while significantly reducing postoperative discomfort and facilitating a faster recovery.
What Happens During Surgery?
All procedures are performed under a general anaesthetic.
Most operations take approximately 1-2 hours, depending on the size and complexity of the hernia. Several small keyhole incisions are used to insert a high-definition camera and specialised instruments.
At the completion of surgery, the wounds are closed with dissolving sutures beneath the skin and covered with waterproof dressings.
Most patients remain in hospital for one night before returning home the following morning.
Recovery After Surgery
Recovery following laparoscopic or endoscopic hernia repair is generally much faster than after traditional open surgery.
Typical recovery milestones include:
- Hospital stay: Overnight
- Walking: Immediately after surgery
- Normal diet: Immediately, with no dietary restrictions
- Return to desk-based work: Approximately 5-7 days
- Driving: Once comfortable, no longer requiring strong pain medication, and able to perform an emergency stop safely (typically within one week)
- Swimming: From approximately 3 weeks, once the wounds have completely healed
- Heavy lifting, gym, contact sport and strenuous physical activity: Usually after 6-12 weeks, depending on the type of repair and individual healing
Light everyday activities, including walking, are encouraged immediately after surgery. Activity can then be gradually increased over the following weeks while avoiding strenuous abdominal loading until the repair has fully healed.
Why Choose a Minimally Invasive Repair?
Modern laparoscopic and endoscopic techniques offer a number of advantages over traditional open surgery, including:
- Smaller incisions and improved cosmetic results
- Less postoperative pain
- Lower risk of wound infection
- Earlier mobilisation
- Faster return to work and everyday activities
- Excellent long-term durability
- Excellent visualisation of the entire abdominal wall, allowing multiple or previously unsuspected hernias to be identified and repaired during the same operation
- Reduced risk of chronic wound complications
By reconstructing the abdominal wall through small keyhole incisions, these advanced techniques achieve strong, durable repairs while minimising surgical trauma and promoting a faster recovery.
If you are considering surgery for a groin, ventral or incisional hernia, or diastasis recti, A/Prof Taylor will recommend the technique best suited to your individual condition, previous surgery and long-term goals.