Laparoscopic Fundoplication for Reflux
What Is Laparoscopic Fundoplication?
Laparoscopic fundoplication is a keyhole surgical procedure used to treat heartburn and gastro-oesophageal reflux disease (GORD).
The operation restores the natural anti-reflux barrier by repairing and reinforcing the valve between the oesophagus and stomach. For most patients, this provides long-term relief from heartburn, regurgitation and other reflux symptoms, while reducing or eliminating the need for acid-suppressing medication.
Fundoplication remains the gold standard surgical treatment for appropriately selected patients with reflux disease. Unlike acid-suppressing medication, fundoplication helps prevent the reflux of all gastric contents, including acid, bile, pepsin and pancreatic enzymes.
When Is Fundoplication Recommended?
Most people with mild reflux can be managed with lifestyle changes and medication. Surgery may be considered when:
- Symptoms are not adequately controlled by medication
- Long-term medication is undesirable or poorly tolerated
- A hiatus hernia is present
- Regurgitation is the dominant symptom
- Reflux has caused complications such as oesophagitis, aspiration or strictures
Successful anti-reflux surgery depends on careful patient selection and thorough pre-operative assessment.
How Does a Fundoplication Work?
An effective anti-reflux valve relies on several components working together, including the lower oesophageal sphincter, the diaphragmatic hiatus, the angle of His and the segment of oesophagus that lies below the diaphragm.
Fundoplication restores these components and improves the function of the lower oesophageal sphincter by reinforcing its external supports.
This reconstruction:
- Strengthens the anti-reflux valve
- Restores the normal relationship between the stomach, oesophagus and diaphragm
- Recreates the angle of His and lengthens the high-pressure zone at the gastro-oesophageal junction
- Helps prevent the stomach from moving back into the chest
The reconstructed valve remains dynamic and relaxes during swallowing, allowing food and fluids to pass normally into the stomach while limiting the abnormal movement of gastric contents into the oesophagus.
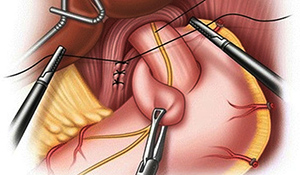
How Is Fundoplication Performed?
The procedure is performed under general anaesthetic using several small abdominal incisions and typically takes around one hour.
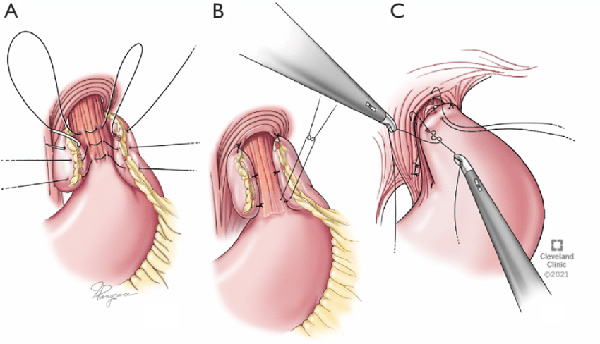
The lower oesophagus and upper stomach are carefully mobilised, the hiatus is repaired and the upper part of the stomach, known as the fundus, is wrapped around the lower oesophagus to reinforce the anti-reflux valve.
The type of fundoplication recommended depends on your anatomy and the results of pre-operative testing.
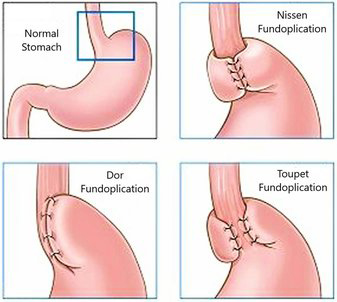
Nissen Fundoplication
A complete 360-degree wrap that provides excellent reflux control and is generally used in patients with normal oesophageal motility. First described in 1955, the Nissen fundoplication remains the benchmark anti-reflux procedure with an excellent long-term track record.
Toupet Fundoplication
A partial 270-degree posterior wrap often preferred for patients with impaired oesophageal motility. It may reduce the risk of post-operative swallowing difficulties and trapped gas while maintaining excellent reflux control.
Dor Fundoplication
A partial 180 to 200-degree anterior wrap most commonly performed alongside a Heller cardiomyotomy for achalasia. In selected patients with significant oesophageal motility disorders, it may also be used as a less restrictive anti-reflux procedure.
What Tests Are Required?
Before recommending surgery, it is important to confirm that reflux is causing your symptoms and assess oesophageal function.
Not all tests are required for every patient. Investigations commonly performed include:
- Upper endoscopy (gastroscopy)
- Oesophageal manometry
- Ambulatory pH or pH-impedance testing
- Barium swallow imaging
- Reflux isotope scan
What Are the Benefits?
Potential benefits include:
- Long-term relief from reflux symptoms
- Reduced reliance on reflux medication
- Improvement in sleep quality and reflux-related respiratory symptoms
- Repair of an associated hiatus hernia
- Improved quality of life
Recovery After Surgery
Most patients stay in hospital for one night and return to light activities within one week.
Temporary swallowing tightness is common during the first few weeks while swelling settles. For this reason, a gradual texture progression diet is recommended during the first six weeks after surgery. The goal is to return to a normal, unrestricted diet once healing is complete.
Post-Operative Diet
A gradual re-introduction of dietary textures over the first 6 weels is needed to allow swelling to settle and the repair to heal without strain.. The typical dietary phases are:
Weeks 1 to 2: fluids of any type
- Soups, juices, smoothies and protein shakes
- Tea, coffee, milk products
Weeks 3 to 4: Purees
- Any pureed foods with a smooth consistency
- Yogurts, Bircher muesli, runny scrambled eggs
Weeks 4 to 5: soft foods
- Soft fish, eggs, tender minced meats and well-cooked vegetables
- Pasta, soft cereals and soft fruits
Weeks 7 and beyond: normal unrestricted diet
- Introduce firmer foods slowly
- Eat small meals and chew thoroughly
- Avoid eating quickly or drinking large volumes with meals
It may take up to 3 months for some patients to be able to eat tougher choices comfortably such as bread and steak, these should be reintroduced cautiously.
Activity Restrictions
Walking is encouraged from the day of surgery. This helps prevent complications such as blood clots and chest infections and can assist with temporary gas-related discomfort.
For the first six weeks, avoid:
- Lifting more than 10 kilograms
- Heavy resistance training, abdominal exercises and high-intensity activities
- Significant pushing, pulling or straining
Office-based work can often be resumed within one week, while physically demanding work may require two to six weeks away from work.
What Are the Risks and Side Effects?
Potential risks and side effects include:
- Temporary swallowing difficulty, particularly with bread or meat
- Bloating, increased wind or difficulty belching
- Recurrence of reflux symptoms
- Bleeding, infection or injury to surrounding structures
Most side effects improve during the first few months after surgery.
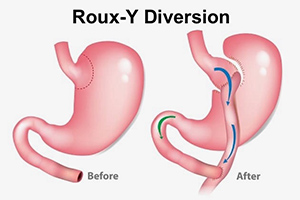
When Fundoplication Is Not Enough: Roux-en-Y Diversion
Although fundoplication is highly effective for most patients, it is not suitable for everyone.
A Roux-en-Y diversion may be considered for selected patients with:
- Severe reflux associated with obesity
- Failed previous fundoplication procedures
- Recurrent reflux after sleeve gastrectomy
- Barrett's oesophagus or complex recurrent hiatus hernias
This procedure creates a small stomach pouch and reroutes part of the small intestine, diverting acid and bile away from the oesophagus. It can provide excellent reflux control when conventional anti-reflux surgery has failed and offers the additional benefit of significant weight loss in patients with obesity.
As this is a more complex operation, it is reserved for carefully selected patients after comprehensive assessment.
Individualised Treatment for Reflux Disease
Anti-reflux surgery is a highly specialised area of upper gastrointestinal surgery. No single operation suits every patient with reflux disease.
The most effective treatment depends on the cause of reflux, the presence of a hiatus hernia, oesophageal function, body weight and any previous surgery.
A/Prof Taylor will provide a comprehensive assessment and determine which investigations and treatment options are most likely to provide safe, durable and effective symptom control.
To arrange an appointment in person or via telehealth, call our office on or book online via HotDoc.