Achalasia
What is Achalasia?
Achalasia is an uncommon disorder of the oesophagus (food pipe or gullet) in which the muscles responsible for moving food from the mouth to the stomach stop working properly.
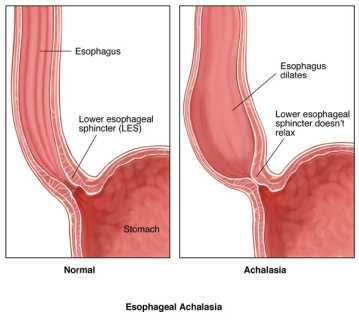
Normally, food is propelled down the oesophagus by coordinated muscular contractions known as peristalsis. At the lower end of the oesophagus sits a muscular valve called the lower oesophageal sphincter (LOS), which relaxes to allow food to enter the stomach.
In patients with achalasia there is a problem with the way the internal nerves within the oesophagus control the muscle; this causes two areas of the oesophagus to function in opposite and conflicting ways: the body of the oesophagus loses its ability to generate normal contractions and becomes flaccid, whilst the sphincter at the bottom of the oesophagus goes into tight spasm and fails to relax. As a result the oesophagus doesn't empty properly leading to progressive swallowing difficulties and other symptoms.
Achalasia is a chronic and unfortunately incurable condition that gradually worsens over time.
What Causes Achalasia?
The exact cause of achalasia remains unknown.
The condition occurs because the specialised nerve cells within the wall of the oesophagus gradually degenerate and stop functioning normally. These nerves are responsible for coordinating oesophageal contractions and relaxation of the lower oesophageal sphincter.
Although the reason for this nerve damage is not fully understood, it is thought to involve an abnormal autoimmune response in genetically susceptible individuals.
Achalasia is not caused by stress, reflux, diet or lifestyle factors.
What Are the Symptoms?
Symptoms often develop gradually and may be present for months or years before a diagnosis is made.
Common symptoms include:
- Difficulty swallowing, especially to solid foods
- Food sticking in the chest after eating
- Regurgitation of undigested food or fluid
- Chest discomfort or chest pain
- Frequent coughing, particularly at night
- Choking episodes during sleep
- Bad breath
- Weight loss
- Recurrent chest infections caused by aspiration
Many patients initially believe they are suffering from reflux disease, however the underlying problem is actually impaired emptying of the oesophagus.
How is Achalasia Diagnosed?
Diagnosis typically involves a combination of investigations.
Upper Endoscopy (Gastroscopy)
Gastroscopy allows direct examination of the oesophagus and stomach. It helps exclude other causes of swallowing difficulties, such as cancer, strictures or severe reflux disease.
Barium Swallow

During this X-ray examination, the patient drinks a contrast liquid which outlines the oesophagus.
Characteristic findings may include a dilated oesophagus with narrowing at the lower end, often described as a "bird's beak" appearance.
Oesophageal Manometry
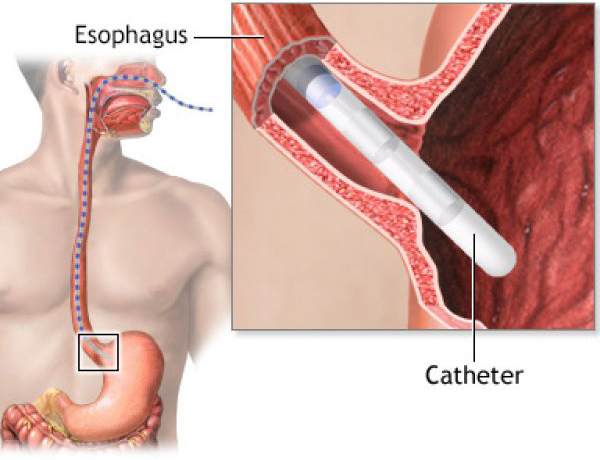
Oesophageal manometry is the most important test for diagnosing achalasia.
A thin catheter is passed through the nose into the oesophagus to measure pressure and muscle function. This test definitively confirms impaired oesophageal contractions and failure of the lower oesophageal sphincter to relax normally.
What Happens if Achalasia is Left Untreated?
Without treatment, symptoms generally worsen over time.
The oesophagus may progressively enlarge and lose function, resulting in increasing difficulty swallowing, malnutrition and weight loss.
Food and fluid retained within the oesophagus can also be aspirated into the lungs, potentially causing recurrent chest infections or pneumonia.
Early treatment usually provides the best long-term outcomes.
Can Medication Treat Achalasia?
Medications generally provide only limited and temporary relief.
Drugs designed to relax the lower oesophageal sphincter are often ineffective and are usually reserved for patients who are not suitable candidates for more definitive treatment.
What Treatment Options Are Available?
The aim of treatment is to overcome the spasm of the lower oesophageal sphincter to improve the emptying of the flaccid oesophagus so food can pass more easily into the stomach.
Balloon Dilatation
A specialised balloon is positioned across the lower oesophageal sphincter and inflated to stretch and partially disrupt the muscle fibres.
This procedure can be effective, although symptoms may recur over time and repeat treatments are often required.
Botox Injection
Botulinum toxin (Botox) can be injected into the lower oesophageal sphincter during endoscopy to temporarily relax the muscle.
While this may provide short-term symptom relief, the effect usually wears off within months and repeat injections are commonly required.
Per-Oral Endoscopic Myotomy (POEM)
POEM is a newer endoscopic procedure performed entirely through the mouth. The inner muscle fibres of the lower oesophageal sphincter are divided without external incisions.
POEM can provide excellent short to medium symptom relief but may be associated with a higher incidence of postoperative reflux.
Laparoscopic Heller's Myotomy
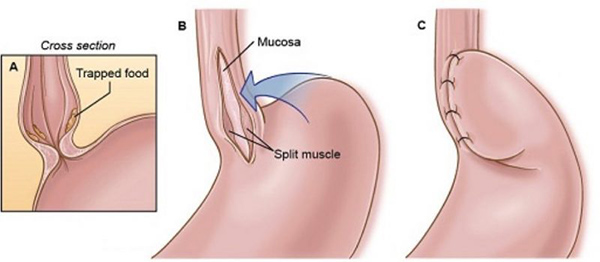
Laparoscopic Heller's myotomy is considered the gold-standard surgical treatment for many patients with achalasia.
Using keyhole surgery, the tight lower oesophageal sphincter muscle is carefully divided, allowing food to pass more freely into the stomach. A partial fundoplication is usually performed at the same time to reduce the risk of postoperative reflux.
This procedure has an excellent long-term success rate and provides durable symptom relief for most patients.
What Results Can Be Expected?
Most patients experience substantial improvement in swallowing following treatment.
Although treatment does not restore normal oesophageal nerve function, it effectively removes the obstruction at the lower end of the oesophagus and significantly improves quality of life.
Long-term success rates following laparoscopic Heller myotomy exceed 90% in many published series.
When Should I Seek Specialist Advice?
You should seek specialist assessment if you experience:
- Difficulty swallowing food or fluids
- Food sticking in your chest after eating
- Regurgitation of undigested food
- Unexplained weight loss
- Recurrent choking episodes or chest infections
- Persistent symptoms despite reflux treatment
Difficulty swallowing should never be ignored and always warrants specialist assessment to exclude serious underlying conditions.
A thorough evaluation by an experienced Upper Gastrointestinal surgeon can determine whether achalasia is present and help identify the most appropriate treatment strategy.
Frequently Asked Questions
Is achalasia cancer?
No. Achalasia is not a cancer and does not become cancer. However, swallowing difficulties can also be caused by cancer, which is why specialist assessment and investigation are important.
Is achalasia hereditary?
Most cases occur sporadically and are not inherited. Rare familial cases have been reported.
Can achalasia come back after treatment?
Symptoms can occasionally recur over time. Fortunately, further treatment options are usually available if this occurs.
Is laparoscopic surgery better than POEM?
Both procedures can be effective, although Heller's myotomy is the gold standard. There are decades of long term data for this procedure. The optimal treatment depends on the subtype of achalasia, patient factors and surgeon expertise. This is best discussed during specialist consultation.