Abdominal Hernia
Abdominal Wall Hernias (Ventral Hernias)
What is an Abdominal Wall Hernia?
An abdominal wall hernia, also known as a Ventral Hernia, occurs when a weakness or defect develops in the abdominal wall, allowing fat or internal organs to protrude through the defect and form a lump beneath the skin.
Ventral hernias are extremely common. They may occur through areas of natural weakness in the abdominal wall or develop following previous abdominal surgery. While some hernias remain small and cause few symptoms, others enlarge progressively over time and may eventually become painful, obstructed or strangulated.
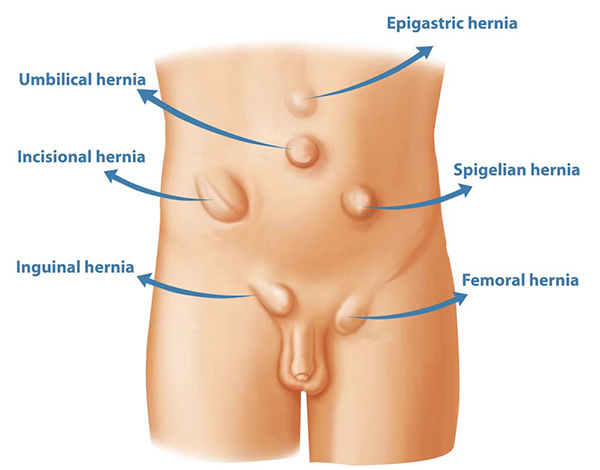
The most common types of ventral hernia include:
- Umbilical and paraumbilical hernias (around the belly button)
- Epigastric hernias (between the breastbone and belly button)
- Incisional hernias (through a previous surgical scar)
Groin hernias, including inguinal and femoral hernias, are discussed separately here.
Types of Ventral Hernia
Umbilical Hernias
Umbilical hernias occur through a natural weakness at the belly button. They may be present from birth or develop later in life as increasing abdominal pressure gradually stretches the tissues around the umbilicus.
Umbilical hernias typically present as a lump at or near the belly button and may cause discomfort, particularly during physical activity.
Epigastric Hernias
Epigastric hernias occur through a weakness in the linea alba, the fibrous tissue that runs down the middle of the upper abdomen between the breastbone and belly button.
These hernias often contain fat and may present as a small, tender lump in the upper midline abdomen. They may be congenital or develop over time due to increased abdominal pressure.
Incisional Hernias
Incisional hernias develop through a previous surgical scar and represent a failure of the healing process. They may develop months or even years after an operation and can range from small defects to very large abdominal wall weaknesses.
Diastasis Recti (Divarication)
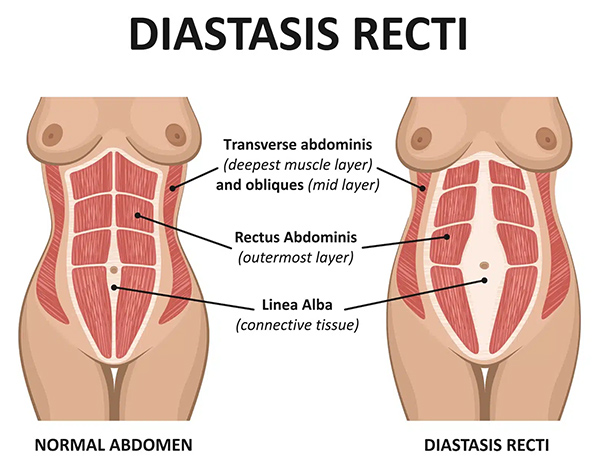
Diastasis recti is not a true hernia but is frequently confused with one. In this condition, the linea alba becomes stretched and widened, causing a broad bulge down the middle of the abdomen, particularly when sitting up or straining. Because there is no actual defect through which abdominal contents can protrude, there is no risk of bowel becoming trapped or strangulated.
However, diastasis recti can cause abdominal wall weakness, poor core strength, cosmetic concerns and discomfort. It is common for an umbilical hernia to coexist with diastasis recti. Divarication is discussed in more detail here.
What Causes Ventral Hernias?
A hernia develops when tissue weakness within the abdominal wall is exposed to increased pressure from within the abdomen. Most patients have a combination of factors contributing to the development of their hernia.
Risk factors for weakness of the abdominal wall include:
- Smoking
- Diabetes
- Advancing age
- Connective tissue disorders
- Previous abdominal surgery
- Steroid medication
Risk factors that increase abdominal pressure include:
- Obesity
- Pregnancy
- Heavy lifting
- Strenuous physical activity and weight training
- Chronic coughing
- Chronic constipation and straining
Can Exercise or Weight Loss Fix a Hernia?
Unfortunately, once a hernia has developed, exercise, physiotherapy and weight loss cannot repair the defect in the abdominal wall. However, weight loss may reduce symptoms, improve fitness for surgery and lower the risk of recurrence following repair.
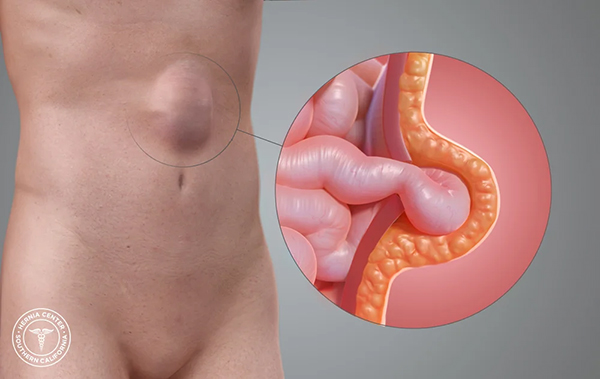
What are the Symptoms of a Ventral Hernia?
The most common symptom is a lump that can be seen or felt within the abdominal wall. A characteristic feature of a hernia is that the lump often fluctuates in size, becoming more noticeable when standing, coughing or straining, and often reducing or disappearing completely when lying down.
Not all hernias are easily visible. Small epigastric hernias, in particular, can be difficult to see or feel and may present simply as localised discomfort or tenderness.
Other symptoms may include:
- Localised discomfort or pain
- A pinching or dragging sensation
- Tenderness over the hernia
- Abdominal bloating
Most hernias gradually enlarge over time, and symptoms often worsen as the defect increases in size. Interestingly, smaller hernias can sometimes be more painful than larger hernias because the contents move through a tighter defect. Exercise and physical activity may become painful.
Are Ventral Hernias Dangerous?
Most ventral hernias are not immediately dangerous. However, hernias do not heal spontaneously and generally become larger over time.
The risk of complications depends partly on the contents of the hernia, with hernias containing bowel generally carrying a greater risk than those containing fat alone.
If a loop of intestine or other abdominal contents becomes trapped within the hernia, this is known as incarceration. If the intestine becomes blocked, a bowel obstruction may occur. If the blood supply becomes compromised, the hernia is said to be strangulated.
A strangulated or obstructed hernia is a surgical emergency requiring urgent treatment.
Symptoms requiring urgent medical attention include:
- Sudden severe pain
- A hernia that cannot be pushed back in
- Redness over the lump
- Nausea or vomiting
- Abdominal distension
How Are Ventral Hernias Diagnosed?

Most ventral hernias can be diagnosed during a physical examination. A characteristic feature is a lump that changes in size with coughing, straining or lying down. The hernia itself can often be felt, and in many cases the underlying defect in the abdominal wall can also be identified.
Imaging may be helpful in selected cases, particularly for larger, recurrent or complex hernias. Abdominal wall ultrasound is a commonly performed investigation because the layers of the abdominal wall and the hernia can be readily visualised. Dynamic assessment during straining can also help identify smaller hernias.
CT scanning is particularly useful for larger or more complex hernias and provides valuable information regarding the size of the defect, the contents of the hernia and the quality of the surrounding abdominal wall.
Treatment
Unlike many medical conditions, hernias do not heal spontaneously. While some small asymptomatic hernias can be monitored, most gradually enlarge over time and ultimately require repair.
External supportive garments such as hernia belts or trusses do not repair the underlying defect or prevent complications such as incarceration. They are therefore rarely recommended other than for temporary symptom relief in patients who are unsuitable for surgery.
Surgical Repair
Surgery is the only definitive treatment for a ventral hernia.
The aim of surgery is to return the herniated tissues to their normal position within the abdomen and repair the underlying defect in the abdominal wall.
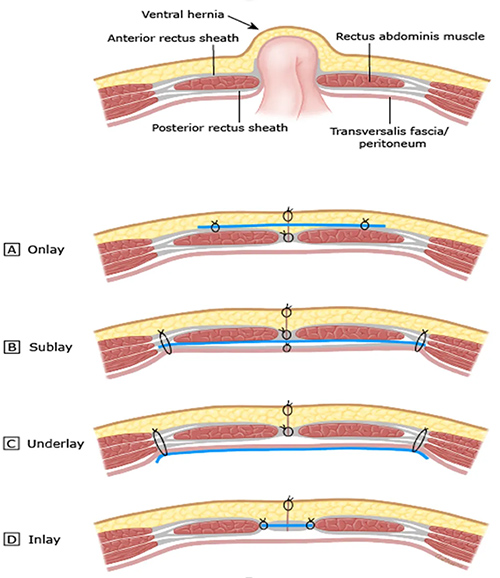
The optimum method of surgical repair will depend on the size, location and complexity of the hernia, but generally a laparoscopic keyhole retro-rectus sandwich mesh repair is preferred for most ventral hernias. Very small umbilical hernias can be satisfactorily repaired by simple sutures. Read more about abdominal wall hernia repair here.
Mesh Reinforcement
In most cases a surgical mesh is used to reinforce the repair and reduce the risk of recurrence.
Mesh acts as a scaffold that strengthens the abdominal wall both directly as well as by promoting additional biological reinforcement by stimulating collagen production as the body's own tissues heal into it. Modern meshes are lightweight, durable and specifically designed for abdominal wall reconstruction.