Superior Mesenteric Artery Syndrome
What is Superior Mesenteric Artery Syndrome?
Superior Mesenteric Artery Syndrome (SMAS), also known as Wilkie's Syndrome, is a rare condition in which part of the small intestine becomes compressed between two major blood vessels within the abdomen.
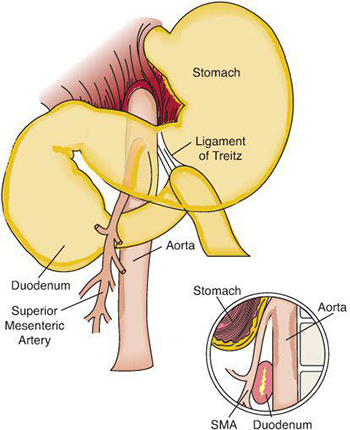
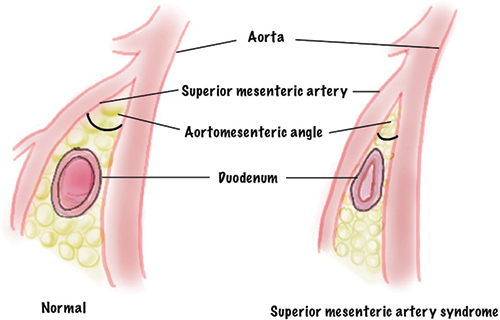
Normally, the third part of the duodenum (the first section of the small intestine) passes comfortably between the aorta and the superior mesenteric artery. A cushion of fatty tissue normally separates these structures and prevents compression.
In patients with SMAS, the angle between these blood vessels becomes abnormally narrow, compressing the duodenum and causing a partial blockage of the digestive tract.
This can lead to difficulty emptying the stomach and upper small intestine, resulting in pain, nausea, vomiting and weight loss.
What Causes Superior Mesenteric Artery Syndrome?
The most common cause is significant weight loss.
Loss of the normal fatty tissue surrounding the superior mesenteric artery reduces the angle between the artery and the aorta, allowing the duodenum to become compressed.
Common situations associated with SMAS include:
- Rapid weight loss
- Severe illness or trauma
- Major surgery
- Eating disorders
- Cancer-related weight loss
- Chronic medical conditions causing malnutrition
- Very low body weight
Less commonly, certain anatomical variations may predispose some individuals to developing the condition.
A vicious cycle often develops whereby weight loss causes duodenal compression, leading to nausea and poor oral intake, which in turn causes further weight loss and worsening compression.
What Are the Symptoms?
Symptoms may develop gradually or occur more suddenly following significant weight loss.
Common symptoms include:
- Upper abdominal pain after eating
- Early satiety (feeling full quickly)
- Nausea
- Vomiting, particularly after meals
- Bloating
- Excessive fullness after eating
- Reflux symptoms
- Unintentional weight loss
- Fear of eating due to symptoms
Many patients notice that symptoms improve in certain positions, such as lying on their left side, lying face down, or bringing their knees towards their chest.
Why is SMAS Difficult to Diagnose?
SMAS is uncommon and its symptoms overlap with many other gastrointestinal conditions.
Conditions that may produce similar symptoms include:
- Gastroparesis
- Functional dyspepsia
- Peptic ulcer disease
- Gallstones
- Chronic pancreatitis
- Gastro-oesophageal reflux disease (GORD)
- Eating disorders
- Intestinal motility disorders
Many patients undergo extensive investigations before the diagnosis is established.
Because narrowing of the aorto-mesenteric angle can occasionally be seen on imaging without symptoms, radiological findings must always be interpreted in the context of the patient's clinical presentation.
How is SMAS Diagnosed?
Diagnosis usually involves a combination of clinical assessment and specialised imaging.
CT Angiography
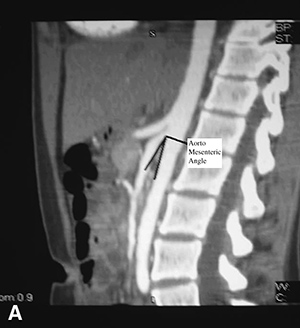
CT angiography is the most commonly used investigation.
The scan can demonstrate narrowing of the angle between the aorta and superior mesenteric artery, along with compression of the duodenum and dilatation of the stomach and proximal duodenum.
Upper Gastrointestinal Contrast Study
A barium meal or contrast study may demonstrate delayed passage of contrast through the compressed segment of the duodenum.
Upper Endoscopy (Gastroscopy)
Gastroscopy is often performed to exclude other causes of upper gastrointestinal symptoms and obstruction.
Additional Investigations
Depending on the clinical situation, gastric emptying studies and other investigations may be required to exclude alternative diagnoses.
What Happens if SMAS is Left Untreated?
Persistent duodenal obstruction can lead to:
- Progressive weight loss
- Malnutrition
- Dehydration
- Electrolyte disturbances
- Ongoing abdominal pain and nausea
- Reduced quality of life
The severity of symptoms varies considerably between individuals.
What Treatment Options Are Available?
Nutritional Rehabilitation
Initial treatment is usually focused on restoring body weight.
Because loss of the fatty tissue around the superior mesenteric artery is often the underlying cause, nutritional rehabilitation may increase the angle between the artery and aorta and relieve the compression.
Treatment may include:
- Dietary modification
- High-calorie nutritional supplements
- Dietitian support
- Enteral feeding via a feeding tube in severe cases
Many patients improve with nutritional therapy alone.
Surgical Treatment: Laparoscopic Duodenojejunostomy?
Surgery is considered when symptoms are severe, nutritional rehabilitation has been unsuccessful, or significant duodenal obstruction persists despite conservative treatment.
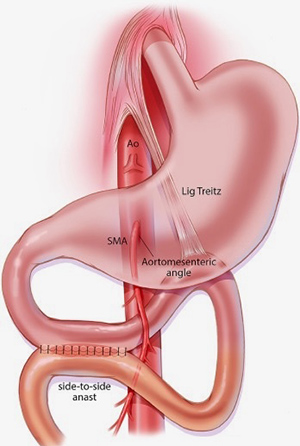
The aim of surgery is to bypass the compressed section of the duodenum and restore the normal passage of food through the digestive tract.
The operation is called a laparoscopic duodenojejunostomy and is performed using keyhole surgery. During the procedure, a new connection is created between the duodenum and the jejunum, the section of small intestine beyond the point of compression. This allows food to bypass the obstruction and pass freely into the remainder of the small bowel.
Laparoscopic duodenojejunostomy is considered the gold-standard surgical treatment for Superior Mesenteric Artery Syndrome and has excellent long-term success rates. Most patients experience significant improvement in symptoms and can return to normal eating following recovery.
Strong's Procedure
Less commonly, division of the ligament of Treitz may be performed to mobilise the duodenum and relieve compression.
This procedure is now performed less frequently than duodenojejunostomy.
What Results Can Be Expected?
Many patients improve with nutritional rehabilitation and weight restoration alone.
For patients requiring surgery, laparoscopic duodenojejunostomy generally provides excellent symptom relief, with published success rates often exceeding 80–90%.
The best outcomes are seen in patients with characteristic symptoms, objective radiological evidence of duodenal compression and exclusion of alternative explanations for their symptoms.
When Should I Seek Specialist Advice?
You should seek specialist assessment if you experience:
- Persistent nausea or vomiting
- Upper abdominal pain after eating
- Significant unexplained weight loss
- Early satiety
- Difficulty maintaining adequate nutrition
- Ongoing symptoms despite normal routine investigations
Because SMAS is uncommon and shares symptoms with many other gastrointestinal disorders, assessment by an experienced Upper Gastrointestinal surgeon is often required to determine whether the diagnosis is likely and whether treatment may be beneficial.
Frequently Asked Questions
Is SMAS common?
No. SMAS is a rare condition.
Can weight loss cause SMAS?
Yes. Significant weight loss is the most common cause of SMAS because it reduces the fatty tissue that normally prevents compression of the duodenum.
Can SMAS improve without surgery?
Yes. Many patients improve with nutritional rehabilitation and restoration of body weight.
Is surgery always required?
No. Surgery is generally reserved for patients who fail conservative treatment or have persistent symptoms and evidence of significant obstruction.
Is SMAS dangerous?
Severe untreated SMAS can result in malnutrition, dehydration and significant weight loss. Fortunately, most patients improve with appropriate treatment.