Heartburn Reflux
What is Reflux?
Gastro-oesophageal reflux disease (GORD) occurs when stomach fluids, including acid, digestive enzymes and bile, flow abnormally back up into the oesophagus.
The most common symptom is heartburn, a burning, rising discomfort in the chest. Occasional reflux after a large, rich or spicy meal, or after excess alcohol, is common and does not necessarily indicate disease. However, when reflux occurs regularly, these gastric fluids can irritate and damage the lining of the oesophagus, causing inflammation and, in some cases, longer-term complications.
Reflux may also travel beyond the oesophagus into the throat, voice box or airways. This is known as laryngo-pharyngeal reflux, or LPR, and may cause symptoms such as voice hoarseness, chronic cough or throat irritation.
What Causes Reflux?
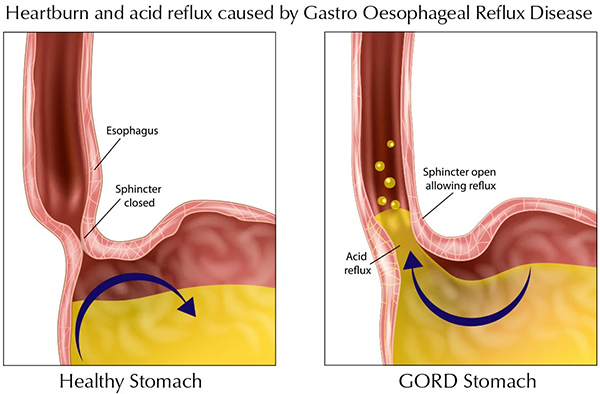
Reflux occurs when the anti-reflux mechanism at the junction between the oesophagus and stomach fails to function properly, allowing stomach contents to flow back into the oesophagus.
GORD can be broadly divided into two categories: structural reflux and functional reflux.
Risk factors for reflux include a family history of the condition, increasing age, obesity (particularly excess abdominal weight), pregnancy, smoking, excessive alcohol consumption, certain medications, disorders affecting gut motility, and a diet high in rich, fatty or spicy foods. Excessive caffeine intake may also contribute to symptoms in some individuals. In many patients, reflux develops as a result of several contributing factors rather than a single cause.
Structural Reflux
Structural reflux occurs when the normal anatomy of the anti-reflux valve becomes disrupted, most commonly by a sliding hiatus hernia. In this condition, part of the stomach and the lower oesophageal sphincter slide upwards through the diaphragm into the chest. This alters the anatomical configuration of the anti-reflux barrier and reduces its ability to prevent reflux. Learn more about hiatus hernias and their treatment.
When a hiatus hernia is responsible for reflux symptoms, surgical repair is highly effective and can provide durable long-term symptom control in appropriately selected patients.
Functional Reflux
Functional reflux occurs when reflux is present despite normal anatomy. In these patients, the anti-reflux mechanism is impaired because the lower oesophageal sphincter is weak, relaxes inappropriately, or because the oesophagus is less effective at clearing refluxed material. Some patients may also have an unusually sensitive oesophagus, causing significant symptoms even when the amount of reflux is relatively small. For patients with proven functional reflux, laparoscopic fundoplication can restore the effectiveness of the anti-reflux valve and provide excellent symptom control. Learn more about reflux surgery and treatment options.
What symptoms does Reflux cause?

Symptoms vary considerably between individual patients, and many patients will have at least 2 of the following:
- Heartburn (a burning sensation rising behind the breastbone)
- Regurgitation of food, foam or bile.
- Bitter metallic taste in the mouth
- Chest tightness (sometimes mistaken for angina)
- Upper abdominal discomfort
- Swallowing difficulties
GORD may also produce "extra-oesophageal" symptoms- this is known as Laryngo-Pharyngeal Reflux and includes:

- Chronic cough (often dry, worse after awaking in the morning)
- Recurrent chest infections
- Wheezing or asthma-like symptoms
- Voice hoarseness
- Sore throat
- Bad breath
- Tooth decay
Some patients may only experience these predominantly respiratory or throat symptoms and may be misdiagnosed as having “adult-onset asthma”. A test called a Reflux isotope scan can help clarify the underlying cause (see below)
Should Reflux be treated?

Persistent reflux may lead to progressive inflammation and damage to the lining of the oesophagus and therefore needs to be taken seriously. Potential complications of chronic reflux include:
- Oesophagitis (inflammation of the oesophageal lining, graded in severity from A to D)
- Ulcer formation
- Iron deficiency anaemia
- Scarring and oesophageal stricture
- Difficulty swallowing
- Barrett’s oesophagus and
- Increased risk of oesophageal adenocarcinoma
- Recurrent chest infections
- Accelerated dental decay
- Loss of voice
How is GORD Diagnosed?
Several investigations are available to diagnose GORD and determine its underlying cause. Assessment typically begins with an upper endoscopy, with further testing tailored according to the patient's symptoms, response to treatment and endoscopic findings.
Upper Endoscopy (Gastroscopy)
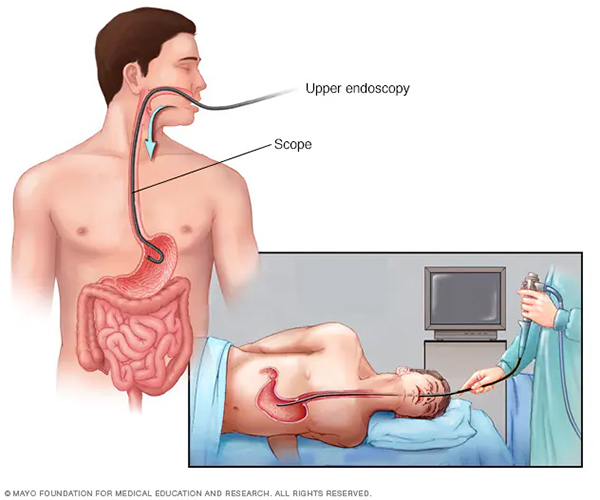
Upper endoscopy is usually the first-line investigation for patients with significant reflux symptoms. During the procedure, a flexible camera is passed through the mouth into the oesophagus, stomach and duodenum, allowing direct visual assessment of the upper gastrointestinal tract.
Gastroscopy can identify complications of reflux including oesophagitis, Barrett's oesophagus, strictures and ulcers. It is also highly effective at detecting a hiatus hernia and excluding other conditions that may mimic reflux, including oesophageal cancer, gastric pathology and achalasia.
The procedure is performed as a day case under intravenous sedation, typically takes less than 20 minutes, and has an excellent safety profile.
Imaging
CT scans, contrast swallow studies and other forms of chest imaging can provide valuable information about the anatomy of the oesophagus, stomach and diaphragm. These investigations are particularly useful for assessing the presence, size and configuration of a hiatus hernia and can assist in planning surgical treatment when required.
Oesophageal Manometry
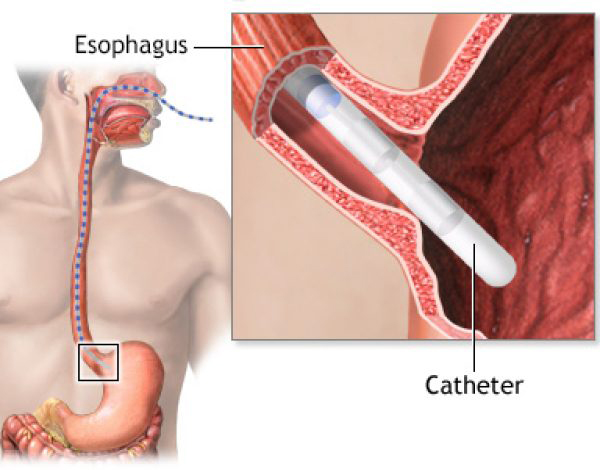
Oesophageal manometry measures the function of the oesophageal muscles and the lower oesophageal sphincter.
The test involves passing a fine catheter through the nose into the oesophagus. Pressure sensors along the catheter record the strength and coordination of oesophageal contractions, as well as the function of the anti-reflux valve.
The procedure usually takes around 10 to 15 minutes and is particularly useful before anti-reflux surgery. It also helps identify other oesophageal disorders, including achalasia and severe motility disorders, which can mimic reflux symptoms.
Ambulatory pH Monitoring
Twenty-four-hour pH monitoring measures acid exposure within the oesophagus over an extended period and is considered the gold standard test for confirming acid reflux.
A thin catheter is positioned within the oesophagus and connected to a small portable recorder. Patients continue their normal daily activities while recording symptoms, meals and periods of sleep. This allows objective measurement of reflux episodes and correlation between symptoms and acid exposure.
pH monitoring is particularly valuable when endoscopy findings are normal or when objective confirmation of reflux is required before surgery.
Impedance-pH Monitoring
Impedance testing is an advanced form of reflux monitoring that can detect both acidic and non-acidic reflux episodes.
Because it measures the movement of fluid and gas within the oesophagus rather than simply acidity, it is particularly useful in patients with persistent symptoms despite acid-suppressing medication. It can identify ongoing reflux even when acid levels have been effectively controlled by PPIs.
The test uses a catheter similar to standard pH monitoring and is usually performed over a 24-hour period.
Bravo Wireless pH Monitoring

The Bravo system is a catheter-free method of measuring oesophageal acid exposure.
During an upper endoscopy, a small capsule approximately the size of a vitamin tablet is temporarily attached to the lining of the lower oesophagus. The capsule continuously records acid exposure and transmits data wirelessly to a portable receiver worn by the patient.
After several days, the capsule naturally detaches and passes harmlessly through the digestive tract.
The principal advantage of Bravo monitoring is improved patient comfort, as no nasal catheter is required. It also allows a longer period of monitoring, typically 48 to 96 hours, which may improve diagnostic accuracy in selected patients. The main disadvantages are the requirement for endoscopy and the higher cost compared with conventional catheter-based pH monitoring.
Treatment of GORD
Treatment depends on the frequency and severity of symptoms, as well as the degree of damage being caused.

Lifestyle Measures
Lifestyle modification can help reduce reflux symptoms and may be sufficient for patients with mild disease. Common measures include:
- Avoiding foods and drinks known to trigger symptoms, such as fatty, rich or spicy foods
- Eating smaller meals
- Avoiding large meals close to bedtime
- Remaining upright for at least two to three hours after eating
- Weight loss, particularly in patients with excess abdominal weight
- Elevating the head of the bed during sleep
- Smoking cessation
- Limiting alcohol intake
While lifestyle measures can improve symptoms, they are often most effective when combined with other treatments in patients with established GORD.
Medication Therapy
If lifestyle measures alone do not provide adequate symptom control, medication therapy is usually recommended.
Antacids
Antacids work by neutralising stomach acid and can provide rapid, short-term relief of symptoms. Common examples include Gaviscon and Mylanta, which are available as liquids and chewable tablets.
While effective for occasional symptoms, antacids do not address the underlying cause of reflux and are generally unsuitable as a long-term treatment for significant GORD.
Acid-Suppressing Medications

Acid-suppressing medications reduce the production of stomach acid and are the mainstay of medical treatment for GORD.
Common medications include:
- Proton pump inhibitors (PPIs) such as Losec, Nexium, Somac and Pariet
- H2 receptor antagonists such as Nizatidine
These medications are highly effective at reducing gastric acidity and increasing the pH of refluxed stomach contents. As a result, they are very effective at relieving heartburn and promoting healing of reflux oesophagitis.
However, it is important to understand that acid-suppressing medications do not prevent reflux itself. The underlying mechanical problem with the anti-reflux valve remains unchanged, meaning stomach contents can continue to reflux into the oesophagus despite treatment.
In addition, PPIs reduce acid but do not eliminate other components of refluxate, including bile salts, pepsin and digestive enzymes. Consequently, some patients continue to experience regurgitation, chronic cough, throat symptoms, voice changes or persistent reflux despite adequate acid suppression.
PPIs are generally safe and well tolerated. However, prolonged long-term use has been associated with an increased risk of certain complications, including nutrient deficiencies, gastrointestinal infections, kidney disease and osteoporosis-related fractures. For this reason, patients should be maintained on the lowest effective dose and reviewed periodically to ensure ongoing therapy remains appropriate.
For patients requiring lifelong medication, those with persistent symptoms despite medical therapy, or those wishing to avoid long-term medication use, anti-reflux surgery may provide an effective alternative by correcting the underlying mechanical cause of reflux.
Laparoscopic Anti-Reflux Surgery
Laparoscopic anti-reflux surgery encompasses two closely related procedures: hiatus hernia repair and fundoplication. Together, these operations restore the normal anatomy and function of the anti-reflux valve, providing effective long-term control of reflux symptoms.
Hiatus Hernia Repair
Hiatus hernia repair is performed when the anti-reflux valve has migrated upwards into the chest as a result of a hiatus hernia. The operation restores the stomach and lower oesophagus to their normal position below the diaphragm and repairs the enlarged opening in the diaphragm through which the hernia has occurred.
The procedure is performed using minimally invasive laparoscopic (keyhole) surgery.
Read more about hiatus hernia repair here.
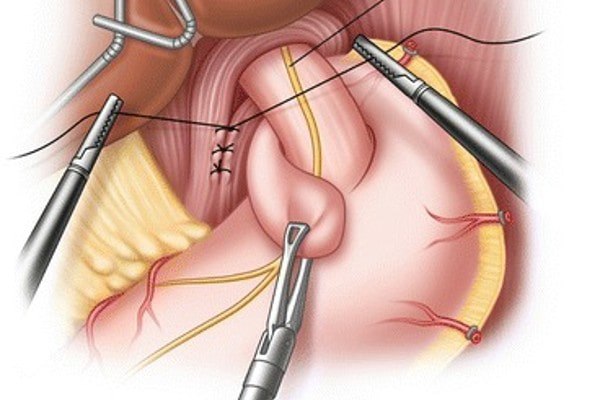
Fundoplication
Fundoplication involves wrapping the upper part of the stomach (the fundus) around the lower oesophagus to reinforce the anti-reflux valve and improve its ability to prevent reflux. Depending on the patient's anatomy and oesophageal function, either a complete (Nissen) or partial (Toupet) fundoplication may be performed.
The procedure is also performed using minimally invasive laparoscopic (keyhole) surgery.
Read more about fundoplication surgery here.
Effectiveness of Anti-Reflux Surgery
Laparoscopic anti-reflux surgery is one of the most effective treatments available for appropriately selected patients with GORD. By restoring the normal anatomy and function of the anti-reflux valve, it addresses the underlying cause of reflux rather than simply suppressing stomach acid.
Numerous randomised controlled trials have demonstrated that anti-reflux surgery provides excellent long-term reflux control, reduces or eliminates the need for ongoing medication, and delivers significant improvements in quality of life when compared with medical therapy alone.