Gastro-oesophageal Reflux Disease
Gastro-Oesophageal Reflux Disease (GORD) What is GORD?
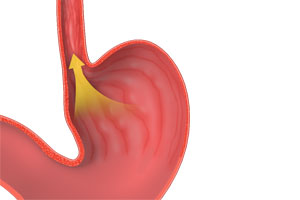
Gastro-oesophageal reflux disease (GORD) is a condition in which stomach contents, including acid, digestive enzymes and occasionally bile-containing fluid, flow abnormally upwards from the stomach into the oesophagus (food pipe). This reflux can irritate and damage the lining of the oesophagus, producing troublesome symptoms and potentially leading to complications over time.
When reflux extends beyond the oesophagus into the throat and voice box, it is termed laryngo pharyngeal reflux (LPR). This can produce symptoms such as chronic cough, throat irritation and voice changes.
Occasional reflux after a large meal, alcohol consumption or lying down is common and does not necessarily indicate disease. However, when reflux becomes frequent, persistent, or begins causing injury to the oesophagus or upper airway, it becomes a disease process that warrants assessment and treatment.
What Causes GORD?

The oesophagus and stomach are connected by a specialised anti reflux barrier located at the lower end of the oesophagus. This barrier consists of several anatomical components working together, including:
- The lower oesophageal sphincter (LOS)
- The diaphragm
- The angle of His
- Supporting ligamentous structures (Phreno-Oesophageal Ligament)
GORD develops when this anti reflux mechanism becomes impaired.
Broadly, reflux may occur due to:
Structural GORD, where normal anatomy is disrupted, most commonly by a hiatus hernia, or
Functional GORD, where the anti reflux mechanism fails despite relatively normal anatomy.
Common contributing mechanisms include:
- Weakening of the lower oesophageal sphincter
- Excessive transient relaxation of the sphincter
- Elevated pressure within the abdomen
- Delayed stomach emptying
- Impaired oesophageal clearance mechanisms
In many patients, GORD frequently results from a combination of factors rather than a single cause.
Risk Factors for GORD
Factors associated with an increased risk of reflux include:
- Obesity, particularly central adiposity
- Hiatus hernia
- Pregnancy
- Smoking
- Excess alcohol consumption
- Large rich meals, particularly late in the evening
- Foods and beverages known to trigger symptoms, including high fat meals and excess caffeine
- Certain medications
- Delayed gastric emptying and gut dysmotility
What Symptoms Can GORD Cause?
Symptoms vary considerably between individuals.
Typical symptoms include:
- Heartburn, a burning sensation rising behind the breastbone
- Regurgitation of food, foamy fluid or refluxate into the mouth
- Bitter or metallic taste
- Upper abdominal discomfort
- Difficulty swallowing
- Food sticking during swallowing
- Chest discomfort or chest pain
Chest pain should always be medically assessed to exclude cardiac causes.
GORD may also produce extra oesophageal symptoms, commonly referred to as laryngo pharyngeal reflux (LPR).
These may include:
- Chronic cough
- Wheezing or asthma like symptoms
- Hoarseness
- Recurrent throat clearing
- Sore throat
- Voice changes
- Bad breath
- Accelerated tooth decay
Some patients experience predominantly respiratory or throat symptoms without significant heartburn and these symptoms may initially be incorrectly attributed to conditions such as adult onset asthma or postnasal drip.
What Happens if GORD is Left Untreated?
Persistent reflux can lead to progressive inflammation and injury of the oesophagus and should not be ignored.
Potential complications include:
- Oesophagitis, inflammation of the oesophageal lining graded from A to D
- Ulcer formation
- Bleeding
- Oesophageal strictures and Schatzki ring formation
- Difficulty swallowing
- Barrett’s oesophagus with intestinal metaplasia
- Increased risk of oesophageal adenocarcinoma
- Aspiration related respiratory complications in selected patients
Not all patients develop complications. However, persistent symptoms warrant appropriate assessment.
How is GORD Diagnosed?
Diagnosis begins with a detailed discussion regarding symptoms, severity, frequency and aggravating factors.
Further investigations may include:
Upper Endoscopy (Gastroscopy)
Gastroscopy involves passing a flexible camera through the mouth into the oesophagus and stomach, allowing direct assessment for:
- Oesophagitis
- Barrett’s oesophagus
- Ulcers
- Hiatus hernia
- Other structural abnormalities
It is typically the first line investigation, takes approximately 20 minutes and is performed as a day procedure under twilight sedation.
Imaging
CT scanning, contrast swallow studies and chest imaging can help identify associated structural abnormalities, including hiatus hernia.
Oesophageal Manometry
Oesophageal manometry measures the strength and coordination of oesophageal contractions and assesses lower oesophageal sphincter function.
The test involves passing a fine catheter through the nose into the oesophagus. Pressure measurements are then recorded throughout the oesophagus during swallowing.
The procedure usually takes approximately 10 minutes and provides valuable information regarding oesophageal motility and valve function.
Ambulatory pH Monitoring
A pH study objectively measures acid exposure within the oesophagus over a prolonged period.
A fine catheter is positioned through the nostril into the lower oesophagus and remains in place for approximately 24 hours while acid levels are recorded. Patients also keep a symptom diary that can then be correlated with reflux episodes.
Impedance Testing
Impedance monitoring detects both acidic and non acidic reflux episodes and can be particularly useful in patients with persistent symptoms despite medication.
It uses a catheter similar to pH monitoring and is generally performed over a 24 hour period.
Bravo pH Capsule
The Bravo capsule is a newer form of reflux monitoring involving a tiny wireless capsule temporarily attached to the lower oesophagus during endoscopy.
The capsule records acid exposure over several days before naturally detaching and passing harmlessly through the digestive tract.
Its principal advantage is improved comfort because it avoids a nasal catheter. However, it requires endoscopy and is generally more expensive than standard catheter based testing.
Reflux Isotope Scan
A reflux isotope scan is a highly accurate test to investigate whether throat symptoms are due to GORD. In this test, a harmless radioactive fluid is consumed, and then a specialised camera is able to see where that fluid ends up over the course of several hours.
A/Prof Taylor will determine which tests are necessary for your individual circumstances based on a careful assessment of your history and arrange them for you.
Treatment of GORD
Treatment is individualised and generally progresses through several stages.
Lifestyle Measures
Simple modifications can significantly improve symptoms and reduce reflux episodes.
These include:
- Avoid foods known to trigger symptoms
- Eat smaller meals
- Avoid eating within three hours of lying down
- Lose weight
- Elevate the head of the bed
- Stop smoking
- Reduce alcohol intake
Medication Therapy
If lifestyle measures alone are insufficient, medication may be recommended.
Antacids
Antacids neutralise existing stomach acid and provide rapid short term symptom relief.
Common examples include:
- Gaviscon
- Mylanta
These are available as liquids and chewable preparations.
Acid Suppression Therapy
Acid suppression medications reduce stomach acid production and allow inflammation to heal.
Common medications include:
- Proton pump inhibitors (PPIs), including Losec, Nexium, Somac and Pariet
- H2 receptor antagonists such as Nizatidine
These medications are highly effective in reducing stomach acidity and healing reflux related inflammation.
However, they do not correct underlying anatomical problems such as hiatus hernia and may not prevent non acidic reflux containing digestive enzymes or bile.
Many patients benefit greatly from these medications, although prolonged use should be periodically reviewed and tailored to individual circumstances.
Potential associations reported with long term use include:
- Reduced nutrient absorption especially Iron and Vit C
- Increased risk of gastrointestinal infections
- Osteoporosis
- Kidney disease
Who May Benefit from Surgery?
Patients considered for anti reflux surgery commonly include those with:
- Proven reflux despite medical therapy
- Hiatus hernia
- Regurgitation poorly controlled with medication
- Medication intolerance
- Barrett’s oesophagus in selected circumstances
- Desire to avoid lifelong medication
Anti Reflux Surgery
For selected patients, surgery may provide the most effective long term treatment.
Modern anti reflux surgery is usually performed using minimally invasive laparoscopic techniques through several small incisions.
The procedure aims to restore normal anti reflux anatomy by repairing associated hiatus hernias and reinforcing the natural valve mechanism between the oesophagus and stomach.
A key component of anti-reflux surgery is fundoplication, where the upper part of the stomach, known as the fundus, is wrapped around the lower oesophagus.
This reinforces the anti reflux barrier by:
- Restoring and accentuating the angle of His
- Augmenting lower oesophageal sphincter pressure
- Reducing the pressure gradient that encourages reflux
- Reconstructing normal anatomy at the junction between the oesophagus and stomach
The operation typically takes approximately one hour under general anaesthesia.
Most patients remain in hospital overnight and can return to office based work within approximately one week.
A temporary texture modified diet is required during early recovery, with gradual return to a normal diet and unrestricted activity over approximately six weeks.